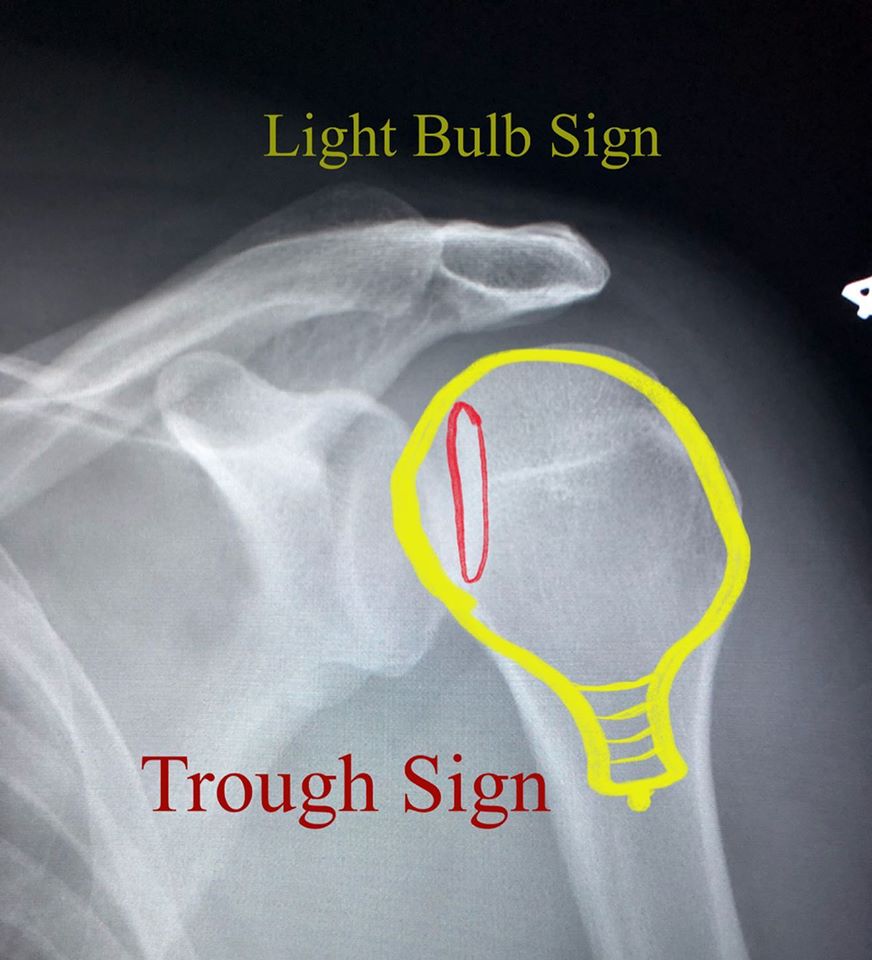
Posterior shoulder dislocation! Although accounting for only 4% of all shoulder dislocations, it’s a commonly missed injury on initial AP radiographs. The mechanism of injury is usually anteroposterior vector trauma to an arm in internal rotation and slight abduction. It’s commonly seen on patients with seizures and during electrocution (not the most common causes but frequently asked on tests!). Anterior shoulder dislocations are much more common (95% of all shoulder dislocations) and much easier to diagnose radiographically. Interestingly, anterior dislocations are much more common because the 45-degree tilt of the scapula and hand-eye coordination. No need to have specialized arm/hand movements on the back, as there are no eyes to coordinate and control them. When the shoulder dislocates anteriorly, it also subluxates inferiorly. In contrast, when the shoulder dislocates posteriorly, it only does so in the posterior direction. This makes a big difference in terms of radiographic evaluation because in anterior dislocation you can see the humeral head not articulating with the glenoid in the AP view mostly because of the inferior subluxating component. We don’t have that benefit on posterior dislocation and the glenohumeral joint often appears congruent on the AP view. The axillary view would greatly help in the diagnosis, but not universally obtained in the ER. It’s important to keep an eye for shoulders fixed in internal rotation (light bulb appearance of the proximal humerus), for the trough line sign (sclerotic line at humeral head at site of impaction fracture) and for a reverse Hill Sachs deformity (impaction fracture of the anterior humeral head). When in doubt, always ask for an axillary or transcapular Y view. Posterior shoulder dislocations are associated to reverse Bankart lesions, posterior capsular injury and rarely rotator cuff tears.