
Case Presentation
A 60 year old man presented with complaints of painful and persistent erection of 2 day duration which started without any sexual arousal. Patient was a known hypertensive since 5 years and was taking treatment regularly. There was no history of trauma or any other known medical illnesses. On examination the penis was tender, rigid and it felt indurated.
What is the Diagnosis?
This patient is suffering from priapism. It is defined as an involuntary, prolonged erection unrelated to sexual stimulation and it is not relieved by ejaculation.
Definition of Priapism?
It is full or partial erection that continues for more than 4 hours beyond sexual stimulation or orgasms or is completely unrelated to sexual stimulation.
What are the types of Priapism?
Types of priapism:
Low-flow or Ischemic or Veno-Occlusive
High-flow or Non-ischemic or Arterial
Stuttering Priapism
In Veno-Occlusive Priapism, there is initial occlusion of venous outflow and subsequent cessation of arterial inflows.The condition is analogous to muscle compartment syndrome. It is an emergency, interventions beyond 48 to 72 hours of onset relieve erection/pain but have little benefit in preserving potency.
In Arterial Priapism, there is unregulated cavernous arterial inflow resulting from disruption of the cavernous arterial anatomy due to formation of arteriolar-sinusoidal fistula. The etiology is usually attributed to trauma. Typically, the corpora are tumescent but not rigid and the penis is not painful. It is not an emergency, spontaneous resolution or response to conservative therapy has been reported in up to 62% cases.
The term Stuttering priapism is used to describe a pattern of recurrent prolonged and painful erections in main with sickle cell disease.
Which is more common among the given types of priapism?
80% to 90% of clinically presented priapisms are low-flow disorders.
What are the symptoms and signs of priapism?
Low-flow priapism: It is usually painful, although the pain may disappear with prolonged priapism. Following are the clinical features:
Rigid erection
Dark blood upon corporeal aspiration
No evidence of trauma
High-flow priapism: Generally not painful and may manifest in an episodic manner. Characteristics of high-flow priapism are as follows:
Adequate arterial flow
Well-oxygenated corpora
Evidence of trauma: Blunt or penetrating injury to the penis or perineum (Eg Straddle injury)
What are various causes of Priapism?
Following figure shows various etiologies of priapism:
Etiologies of Priapism
What history to take in Priprism?
Duration of erection
H/O Pain
H/O Previous Episodes
H/O Sexual Arousal/ Intercourse
H/O Erectogenic Medication Intake
H/O Drug Abuse
H/O Blood Dyscrisias eg Sickle Cell Disease, Hemoglobinopathies, Hypercoagulable states
H/O Trauma
H/O Other Neurological deficits
How to evaluate a case of Priaprism?
Routine Investigations: CBC, Coagulation Profile, Peripheral Smear (To rule out hematological abnormalities)
Corporal Blood Gas by Aspiration: To differentiate between Veno-Occlusive and Arterial Priaprism
Color Duplex Doppler USG of Penis and Perineum: Veno-Occlusive priapism shows no blood flow, Arterial Priapism shows normal to high blood flow velocities
Penile Arteriography: Reserved for management of high flow priapism when embolization is planned
MRI: May help in 3 ways 1) Imaging of a well-established arteriolar-sinusoidal fistula 2) Identifying corporal thrombus 3) Identifying corporal metastasis
What are the blood gas values in Low flow/ Ischemic Priapism?
PO2: < 30
PCO2: > 60
pH: < 7.25
What is the management of Priapism ?
Following algorithm can be followed for the management of pripism
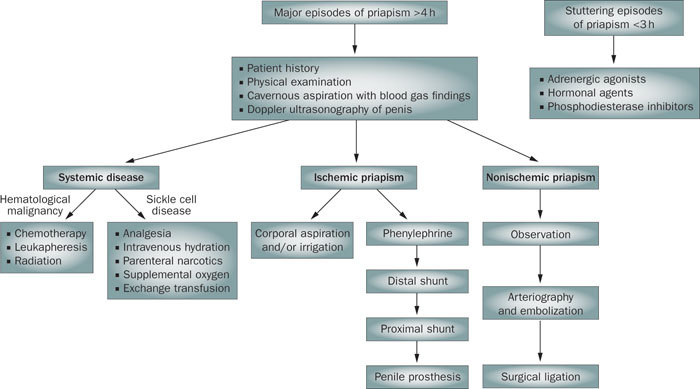
Initial treatment of choice for Ischemic Priapism is Decompression of corpora cavernosa by Aspiration (large bore 19G needle inserted at penoscrotal junction at 3 or 9 o’ clock position. It will soften the erection and relieve pain. It is repeated until no more dark blood is seen coming out. Aspiration alone relieves priapism in 36% cases.
Aspiration if not successful should be followed by injection of a Alpha adrenergic receptor agonist. Phenylephrine is the agent of choice with selective alpha1 adrenergic actions and it lacks Beta mediated ionotropic and chronotropic side effects
Surgical Management of ischemic priapism is done after repeated penile aspirations and injections have failed or such attempts have resulted in cardiological side effects
What are various surgical options for Priapism after conservative management has failed?
Surgical management options in Ischemic Priapism:
Shunting
Immediate Penile Implant
Options in management of Arterial (High Flow) Priapism:
Interventional Angiography (Embolization)
Surgical Ligation of AV fistula
References
Campbell-Walsh Urology: Expert Consult Premium Edition: Enhanced Online Features and Print, 4-Volume Set, 10e
Priapism – Etiology, Pathophysiology And Management, C. Van Der Horst, Henrik Stuebinger, Christoph Seif, Diethild Melchior, F.J. Martínez-Portillo, K.P. Juenemann